
By Hagop Kantarjian, M.D.
Nonresident Fellow in Health Policy, Baker Institute
Mary Alma Welch
Physician Assistant
Nadim Ajami, Ph.D.
Virologist and microbiologist
Status of the Covid-19 pandemic
The Covid-19 pandemic is still in the early-to-mid phases in most of the world. It may continue to spread over at least the next several months or even longer, infecting millions, killing tens of thousands, paralyzing international economies and industries, and altering social fabrics.
The most important questions in the minds of people worldwide are: 1) how do we know when we can get back to a “new normal”? And 2) what will this new normal look like? As of April 14, 2020, Covid-19 has infected 2 million+ people and caused the death of 120,000+.
There are still important unknowns that will influence the final toll of Covid-19: 1) Will it recur in several waves? 2) Will subsequent waves be more or less virulent? 3) Do we develop solid protective immunity after exposure? And 4) how quickly can we develop safe and effective vaccines and drugs to eliminate the virus and reduce the severity of the disease?
To move forward, we need to understand two important concepts: “herd immunity” and the IgG antibody immune response to Covid-19.
“Herd immunity” and its meaning with Covid-19
“Herd immunity” is a term used to describe the idea that viral spread is controlled once a proportion of a population becomes immune, through either exposure to the virus or vaccination. The percentage required depends on the infectivity of a virus and the availability of an effective vaccine. Regular influenza transmits from one person to 1.2 others. Covid-19 is much more contagious and transmits from one person to 6-7 without social protections, and to 2-3 with distancing precautions. It is estimated that 60% of the population should become immune (through exposure or vaccines) to control Covid-19. A study from Iceland conducted testing on 18,000 individuals by nasal swabs and found 1% to be infected, 50% of them without any symptoms. The rate of infected people who are asymptomatic may range from 25% to 50%. There is an important distinction between “clinical infection” and “exposure.” To estimate the rate of “clinical infection,” wide testing with nasal swabs is needed to detect actively infected people. To estimate the rate of “exposure,” blood serology testing is needed to detect the virus-specific IgG antibody that kills the virus (see explanation later). To achieve 60% herd immunity, 60% of a particular population must have a positive serology for the IgG. Only then can anti-Covid-19 measures be relaxed.
Compare this with the reality that apparently less than 1% or the world population has been found to be “infected,” probably due to limited nasal swab testing, mostly of those exhibiting symptoms. Because the antibody test just became available in the United States in the past two weeks, we have no idea yet of the extent of “exposure.” If it is true that only 1% of the world population is so far exposed or infected, then measures to flatten the Covid-19 pandemic curve will only reduce the viral spread to a “slow-motion” pandemic that may simmer at low levels, but explode anytime social precautions are lifted. This is already seen in countries that controlled the Covid-19 spread effectively, then relaxed the social protective measures (South Korea, Singapore, Taiwan, and Hong Kong). Think of it as though it is a wild fire that smolders and spikes until such vast expanses are consumed that it has no more fuel. So we may be consumed by this Covid-19 plague for significantly longer, unless vaccines and drugs are developed soon. Or unless we are pleasantly surprised to find by wide serology testing (IgG) that herd immunity is developing at an unexpectedly fast rate.
Importance of Covid-19 testing
Early and wide Covid-19 testing, coupled with isolation of infected individuals and protective social measures (hygiene, city lockdowns, social distancing) have produced significantly outcomes, measured so far by lower infection and mortality rates, mostly manageable hospital capacities, and optimal medical management. This has been discussed in previous Baker blogs. The US is still early in the Covid-19 pandemic and was affected by delays in Covid-19 testing and protective measures. As of April 13, 2020, 575,000+ Americans were infected (infection rate 0.17%) and 22,000+ have died (mortality rate 3.8%). In such outbreaks, a delay of control measures by one week can triple an epidemic size and prolong it by one month.
Explaining the types of Covid-19 testing
Covid-19 testing obtained by a nasal swab (PCR testing) identifies people with an active SARS-CoV-2 infection about 60%-80% of the time (~20%-40% false negative as discussed before). But it is estimated that 25%-50% of infected people have no symptoms, and they are not being tested at present. People with positive nasal swabs for Covid-19 who have mild or no symptoms should self-quarantine for at least 2-3 weeks (until signs and symptoms resolve completely), and then be tested again to make sure the virus is no longer present. If they are moderately or severely ill, they should be hospitalized, isolated and treated. This test give results in five minutes, using small portable devices that can be deployed widely in all health-care facilities. During Covid-19 high risk period, this test needs to be scaled to allow millions of tests daily.
Covid-19 testing in the blood (serology) involves measuring the immune response of the body to the viral exposure. An early response produces a non-specific immunoglobulin antibody called IgM (first-line but poor defense system). The second, more important anti-Covid-19 response produces a virus-selective IgG antibody, which kills the virus and may provide long-lasting immunity and potential resistance to second Covid-19 infections. Serologic testing for anti-Covid-19 IgG is what defines the rate of exposure to the virus and determines herd immunity. It should be scaled immediately to allow testing of millions daily in the U.S. and the world.
Based on these tests, people can be separated into “Covid-19 immunity profile” groups (see Figure 1). The first are those with no symptoms, and who are Covid-19 negative by both nasal and serologic tests. These individuals have not been exposed and are still at risk. The second are those with positive PCR nasal swabs. These are infected and can infect others. They must be isolated to avoid the viral spread. The third are those who have recovered from a Covid-19 infection, and have developed IgG antibodies (positive serology). These individuals are probably resistant to a reinfection during the same wave (and perhaps a later one). They protect others as buffers in crowds. They may be able to donate plasma (rich with anti-COVID–specific IgG) to treat severely ill patients. They can also safely return to work, and, if they are health-care workers, can be deployed preferentially to treat infected patients. Hence the need for broad testing to understand the patterns of infectivity and herd immunity.
Figure 1. Covid-19 “Immunity Profile” Groups
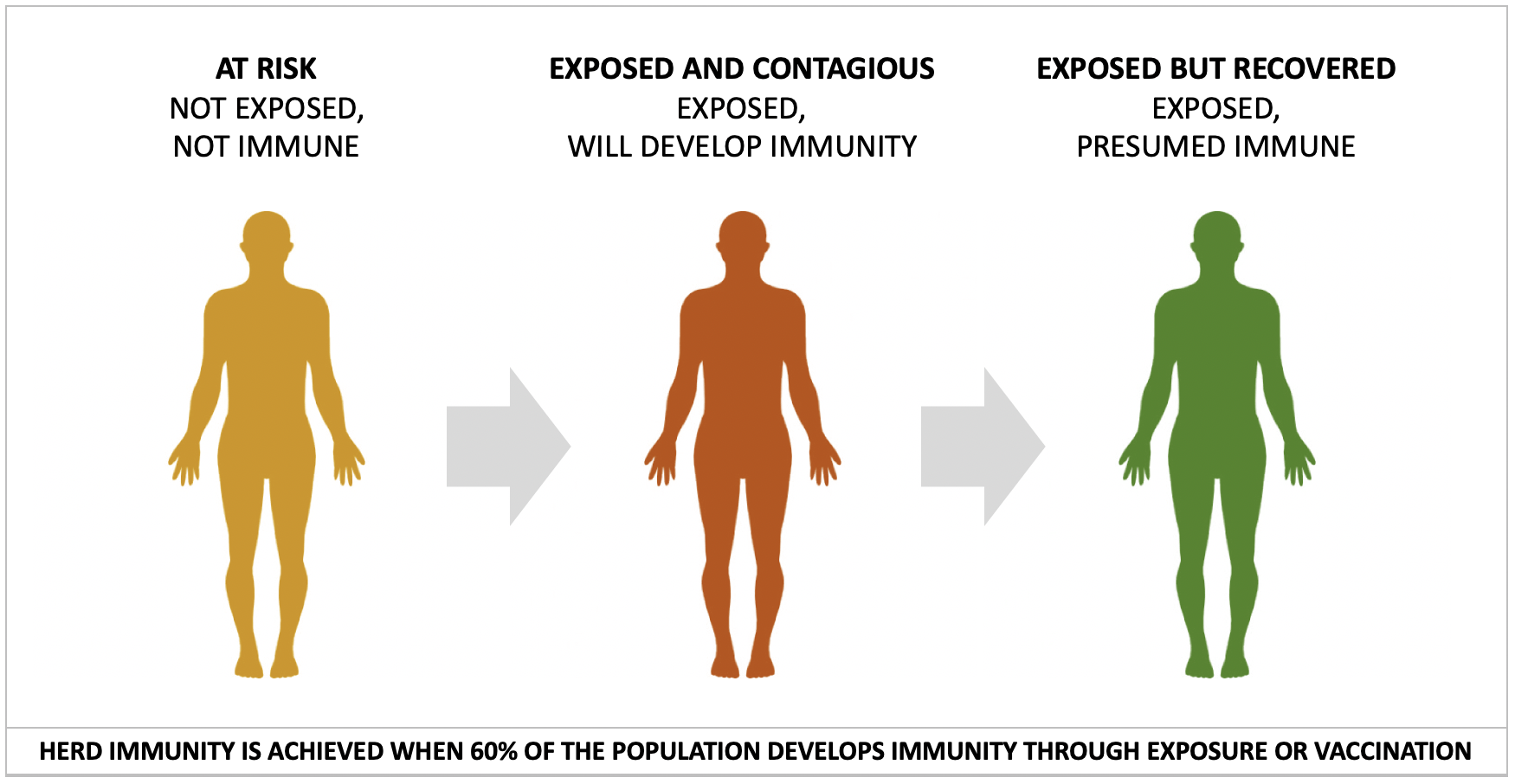
Source: Authors
Defining different Covid-19 risk groups can be used to prevent Covid-19 spread, protect and treat patients, reinvigorate industries and workplaces, and reopen and normalize societal venues.
When will we see the light at the end of the Covid-19 tunnel?
The Covid-19 pandemic can be temporarily suppressed with widespread testing and social protective measures. But the true light at the end of the Covid-19 tunnel and a return to a new normal can only occur with one of the following:
- Herd immunity through exposure to Covid-19 that covers 60% of people. The current infection/exposure estimates are less than 1%-2%. Therefore, testing, isolation and protection measures will flatten the infection spread, likely resulting in many months of a “slow-motion Covid-19 wave” that will spike again as soon as these measures are relaxed.
- Development of effective and safe vaccines. These are the ultimate strategies that will provide broad herd immunity and eliminate Covid-19.
- The development of effective anti-Covid-19 treatments. This is akin to the control of the AIDS epidemic, where no vaccine has been successful, but highly effective therapies are available.
- With luck, the Covid-19 virus will develop mutations that weaken it (as happens with influenza). Or hopefully it will be suppressed by warmer, humid weather, which may result in seasonal epidemics but will allow time to develop vaccines and therapies.
What might life post Covid-19 be like?
The new normal may involve frequent testing of large numbers of the population during periods at high risk of Covid-19 outbreaks. Covid-19 testing may become routine, like measuring blood pressure, temperature and blood counts. People with even very mild symptoms must be tested with nasal swabs. Additionally, all individuals should have a serology test once, then periodically thereafter to monitor IgG status. Testing in medical facilities should be more intensive than in other areas; there is an added responsibility to implement optimal measures that prevent the spread of Covid-19 among patients, health care workers, and their family and social contacts.
The new normal should also include:1) a change in behavior to promote continuation of better hygiene and social distancing; 2) expansion to a system of universal health insurance to allow equal access to high-quality medical care; 3) maximizing the concept of telecommuting and virtual meetings (which should have an added benefit of reducing the footprint of global warming); 4) eliminating the inexorable spread of unnecessary bureaucracies that have paralyzed business and commerce and increased costs 3-10 fold without improving safety or quality (for example, in health care); and 5) continuous and nimble preparations for other pandemics or catastrophic events that may threaten our world.
About the authors
Hagop Kantarjian, M.D., is a medical oncologist and a nonresident fellow in health policy at the Baker Institute. His opinions do not reflect those of his institution affiliation.
Mary Alma Welch is a physician assistant in Houston. Her opinions do not reflect those of her institution affiliation.
Nadim Ajami, Ph.D., is a virologist and microbiologist who specializes in virome and microbiome research. His opinions do not reflect those of his institution affiliation.